Table of Approved ATMPs


Explore available CAR therapies, differentiation, development challenges, and lessons learned.
Would you like to familiarise yourself with CAR Therapies? Watch the replay to explore CAR-based Cell Therapy with our scientist, Somayeh Rezaeifard, elaborating on the various available CAR therapies, their differentiation, current challenges in therapy development, and lessons learned until today.
Whether you’re part of an academic research group, pioneering a new biotech, or working at a global CGT leader, this webinar brings together various aspects of CAR therapies to explore, discuss, and learn.
Key Learnings
Join the conversation and equip yourself with the latest knowledge and insights in CAR-based immunotherapy.

iPSC reprogramming and transdifferentiation both offer exciting opportunities in cell biology. Learn how these approaches are revolutionising regenerative medicine and cell therapy.
Cellular reprogramming is a process by which an adult, specialised somatic cell is transformed into a pluripotent state—an iPSC (induced pluripotent stem cell). These stem cells can differentiate into any cell in the body.
As such, cellular reprogramming presents new opportunities in personalised medicine, disease modelling, and tissue regeneration and represents a monumental step towards a future in which we can alter cellular identities to combat diseases and enhance human health.
iPSCs are stem cells reprogrammed from fully differentiated cells, such as skin or blood cells. While the ability of hiPSCs to differentiate into virtually any cell type is a fundamental characteristic, it’s important to distinguish this from the actual process of hiPSC reprogramming. Reprogramming refers to the initial conversion of differentiated adult cells into pluripotent stem cells. The differentiation of these reprogrammed cells into various cell types, similar to what embryonic stem cells can do, is a separate phase that follows the reprogramming. This distinction is crucial for understanding the scope and potential applications of hiPSC technology in research and clinical settings.
iPSCs have generated interest in stem cell research for several reasons:
Origin from Patient-Specific Cells: hiPSCs can be derived from an individual’s cells, reducing the risk of immune rejection when used for transplantation.
Disease Modelling: Researchers can create hiPSCs from patients with genetic disorders or diseases and study disease mechanisms at the cellular level to screen potential drug candidates.
Regenerative Medicine: By differentiating into tissue/organ-specific cell types, hiPSCs hold the potential to replace damaged or malfunctioning tissues and organs, providing tailored solutions for patients.
Ethical Advantages: iPSCs circumvent some ethical concerns associated with embryonic stem cells, as they do not require the destruction of embryos for their generation.
While iPSCs offer numerous advantages in stem cell research and regenerative medicine, they also come with certain disadvantages and challenges that need to be addressed.
Tumorigenic potential: Tumorigenic potential in iPSCs is linked to genetic and epigenetic memory and differentiation efficiency. Incomplete differentiation, where some cells remain undifferentiated, increases the risk of tumour formation. To mitigate these risks in iPSC-based therapies, it’s crucial to ensure complete and efficient differentiation.
Genetic & Epigenetic Variability: Although we already discussed genetic and epigenetic modifications previously, it’s important to clarify that such changes can arise during the reprogramming process, during subsequent cell culture, or even pre-existing in the donor somatic cells. Each source contributes uniquely to the variability observed in iPSCs, impacting their behaviour and differentiation capacity.
Inefficiency & Variability: Generating iPSCs can be inefficient, with a relatively low success rate in some cases.
Immunogenicity: While hiPSCs generated from a patient’s cells can reduce the risk of immune rejection, there may still be immune responses against hiPSC-derived cells sometimes induced for ex-vivo cell culture
Time & Cost-Intensive: The generation and characterisation of iPSCs are time-consuming and costly processes.
Ethical Considerations: Although reprogrammed cells are an ethical alternative to embryonic stem cells, there are still ethical considerations related to their use, specifically involving manipulating human genetic material.
Viral Vector-based: Viral vector-based reprogramming can involve various types of viruses. While lentiviruses and retroviruses can integrate reprogramming factors into the host cell’s genome, raising concerns about genomic integration and tumorigenicity, adenoviruses are also used in reprogramming. Importantly, adenoviruses do not integrate their genetic material into the host genome, potentially reducing these risks.
mRNA-based: mRNA-based reprogramming uses synthetic messenger RNA (mRNA) to deliver reprogramming factors in a non-integrative manner, which is safer in terms of avoiding genome alteration. Although this method typically involves transfection, mRNA can be introduced into cells through other techniques, broadening its application. However, it is generally considered less efficient than viral methods.
Protein-based: Direct delivery of reprogramming factors as proteins overcome genomic integration concerns, but it may require optimisation to enhance reprogramming efficiency.
Small Molecule-based: Small Molecule-based reprogramming involves using small molecules that can mimic the functions of reprogramming factors, offering an alternative strategy to induce pluripotency. While this approach is less well-established than other methods, it reduces complexity. However, it’s important to note that these small molecules can induce reorganisation of the host genome, which may have safety implications.
The choice of delivery method depends on the specific goals of the research or clinical application, and factors such as efficiency, safety, and potential genomic alterations must be considered.
In contrast to iPSC reprogramming, which involves reverting a specialised cell type to a pluripotent state before differentiating it into another type, transdifferentiation consists of redirecting one specialised cell type directly into another, bypassing the pluripotent stage entirely.
Transdifferentiation is initiated by a combination of changes in gene expression patterns, including specific transcription factors, signalling pathways, and epigenetic modifications. These factors work together to redirect a specialised cell type into another without reverting to a pluripotent state.
iPSC reprogramming and transdifferentiation are two distinct approaches in cellular biology, each with notable differences. As summarised in this image in Nature, these methods alter cell states, specifically geared towards applications in regenerative medicine and cellular therapy.
iPSC reprogramming involves converting a differentiated (adult) cell, such as a skin cell, into a pluripotent stem cell.
Transdifferentiation, or direct reprogramming, takes a different approach. It involves converting one type of adult cell directly into another without the need for a pluripotent stage.
Both iPSC reprogramming and transdifferentiation methodologies have made remarkable progress in a short amount of time, but still face challenges. The current limitations of iPSCs and transdifferentiation include the risk of tumorigenicity, genetic and epigenetic variability, and the need for further optimisation to enhance efficiency.
Future prospects for iPSC reprogramming and transdifferentiation are promising due to ongoing advancements in understanding the underlying molecular mechanisms and improving the technologies. Researchers are continually developing safer and more efficient methods, which could lead to breakthroughs in personalised medicine, disease modeling, and regenerative therapies. As these techniques become more refined, their potential to transform medical treatments and outcomes becomes increasingly feasible.
The integration of emerging technologies and innovative approaches will undoubtedly continue to shape the future of these transformative fields.
The remarkable ability to alter a cell’s identity through induced reprogramming and transdifferentiation has ushered in a new era of science.
However, it must also recognise the challenges that lie ahead. We can overcome these obstacles through collaboration, dedication, and continued advances and fully harness the potential of cellular reprogramming.
At NecstGen, we are at the forefront of pioneering CGT research. To learn how we can help with your development and manufacturing of stem cell and gene therapies, reach out to discuss your challenges.
In these figures, we gathered and visualised overviews of approved ATMPs over the past years for you.

From idea to treatment, you’ll face changing requirement and development challenges. View the figure to see how knowledge of the process inversely relates to freedom to make changes to your process.
")
Our experts are only a message away to help you understand the impact of any of these aspects and make informed decisions on outsourcing.
We’d be happy to discuss and help you bring cell therapies to patients.
Human induced pluripotent stem cells (iPSCs) offer great potential for the future of medicine. We look into the world of human iPSCs, exploring their incredible promise and the critical significance of directing their development towards specialised cell lineages.
Induced Pluripotent Stem Cells (iPSCs) are stem cells generated by reprogramming somatic (adult) cells to return to a pluripotent state. They possess similar attributes to embryonic stem cells (ESCs).
Human iPSCs (hiPSCs) can be differentiated into virtually any cell type found in the human body, using specific growth factors, cytokines, and substrates into mature cells.
Differentiation of hiPSCs compiles a series of steps that mimic tissue and organ formation during embryonic stages.
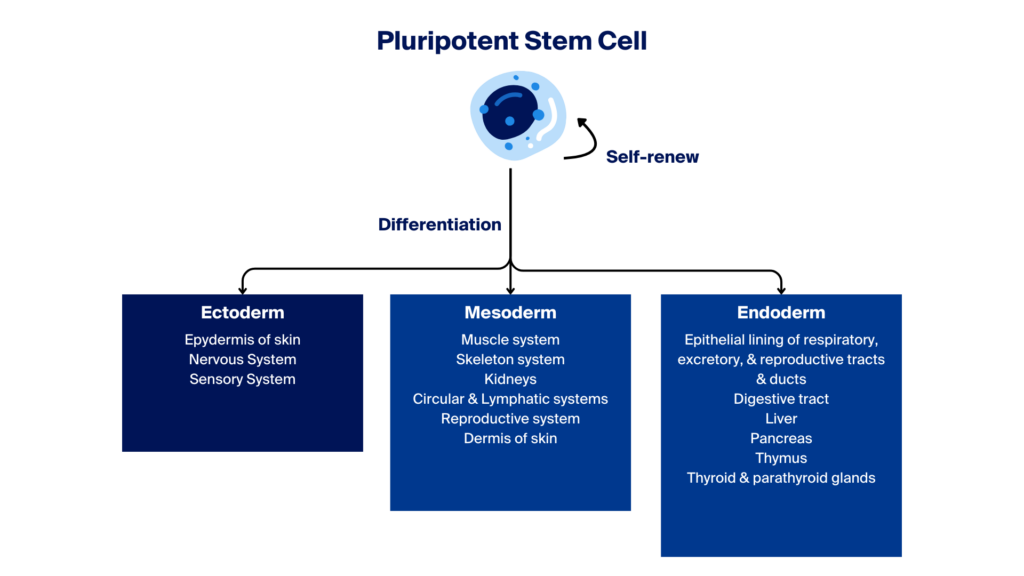
Newly formed pluripotent stem cells (PSCs) have the potential to differentiate into one of three embryonic germ layers—ectoderm, mesoderm, or endoderm—which can further develop into intermediate or terminally differentiated specialised cells.
Differentiation refers to the processes or stages in which iPSCs abandon their pluripotent stage and become committed to line-specific adult-like cell types, which can potentially be used in research and clinical applications.
Various external factors must influence iPSCs’ change for them to successfully undergo the various stages of differentiation.
Growth factors and cytokines are used as signalling molecules that govern the fate of iPSCs directing them along developmental trajectories.
Growth factors such as BMPs, FGFs, and Wnts orchestrate the activation of specific signalling pathways and the expression of lineage-specific genes.
Cytokines influence the behaviour of iPSCs, although not all differentiation processes depend on these external factors for successful specialisation. For instance, interleukin-6 (IL-6) can influence the differentiation of iPSCs into certain immune cells, demonstrating the specific effects of cytokines in stem cell biology.
3D culture systems and organoids offer a physical and structural advantage in replicating in vivo conditions and, in some cases, can enhance the efficiency of iPSC differentiation.
Unlike traditional 2D cultures, these three-dimensional environments provide iPSCs with spatial cues and interactions that more closely mimic native tissues. This fosters accurate differentiation and encourages the formation of complex tissue structures formed by two or more cell types, enabling the study of organ-specific functions and diseases.
Co-culture techniques involve growing iPSCs in the presence of other cell types or within a specific cellular microenvironment.
In some co-culture systems, iPSCs are grown directly with other specific cell types to promote differentiation. This approach aims to mimic the natural cellular interactions and signals in the body, enhancing the differentiation, maturation, and functionality of the iPSC-derived cells. On the other hand, when co-cultures involve cell types from different organs, removing the nurturing cell type component is necessary if cells are intended for functional studies or clinical use.
IPSC differentiation aims to transform iPSCs into specific, functional cell types. This differentiation is essential for advancing regenerative medicine, disease modelling, and drug discovery. The lineages described below are highlighted due to their broad applications and significant impact in current research and therapy development. However, it’s important to note that other lineages, such as lymphopoietic lineages which are crucial for producing allogeneic CAR T cells, also play critical roles in medical science.
Neural Lineages – Initially, hiPSCs are guided to adopt an ectodermal fate, the germ layer from which the nervous system originates. Subsequently, they can be coaxed into neural progenitor cells and further differentiated into mature neurons, astrocytes and glial cells.
Cardiovascular Lineages – The differentiation of hiPSCs into cardiovascular lineages, including cardiomyocytes, smooth muscle cells, endothelial cells and cardiac fibroblasts, involves sequential steps that lead hiPSCs towards a mesodermal fate, the precursor to heart cells. Activation of specific cardiac transcription factors eventually yields functional components of the cardiovascular system.
Hematopoietic Lineages – hiPSCs can be differentiated into various blood cell types, such as erythrocytes, platelets, and immune cells, mimicking the hematopoietic lineage. The process commences with hiPSCs adopting a mesodermal fate and progressing towards hemangioblasts, common precursors for endothelial and blood cells.
Endodermal Lineages – hiPSCs can be directed towards endodermal lineages to generate cell types found in internal organs like the liver and pancreas. The result is the production of functional hepatocytes, pancreatic beta cells, and other organ-specific cell types.
Mesenchymal Lineages—Mesenchymal stem cells (MSCs) derived from hiPSCs are developed by guiding iPSCs towards a mesodermal fate. These cells can differentiate into osteoblasts, chondrocytes, and adipocytes. iPSC-derived MSCs provide a potentially unlimited supply for both autologous and allogeneic cell therapies, overcoming the limitations of donor-derived MSCs.
Although the differentiation of hiPSCs into various cell types holds tremendous potential for regenerative medicine, disease modelling, and drug discovery, the processes involved in iPSC differentiation face several challenges and limitations that researchers are actively working to overcome.
One of the foremost challenges in iPSC differentiation is ensuring the purity of the resulting cell populations.
Although iPSCs possess the remarkable capacity to differentiate into various cell types, this pluripotency can lead to a heterogeneous mix of cells. Researchers face the intricate task of refining differentiation protocols to obtain homogenous populations of desired cells while minimising the presence of off-target cell types.
This complexity necessitates constantly optimising differentiation protocols and novel cell sorting and enrichment techniques.
Another significant challenge is replicating the conditions and timelines of natural human development in vitro.
In vivo development is a finely tuned process influenced by a multitude of factors, including spatial and temporal cues, signalling pathways, and epigenetic modifications. Recreating these intricate dynamics in a culture dish is a formidable task.
Researchers must develop precise differentiation protocols that mimic the in vivo microenvironment to accurately guide iPSCs toward the desired cell fate.
Beyond appearances, it is vital to ensure that the differentiated cells do not merely look the part but also function effectively and safely when transplanted.
Functional validation is a critical aspect of iPSC differentiation. Researchers need to assess differentiated cells’ functionality, maturity, and stability through rigorous quality control measures and functional assays, thus ensuring that iPSC-derived cells can perform their intended roles in therapeutic applications or disease modelling.
With induced pluripotent stem cell (iPSC) research moving rapidly, researchers are actively exploring innovative approaches and leveraging cutting-edge technologies to develop more efficient, scalable, and precise differentiation processes.
Advanced cell culture systems represent a significant avenue of progress. Researchers are working to enhance culture substrates, employ three-dimensional (3D) culture techniques, and use microfluidic systems to better mimic the native microenvironment of developing tissues and organs.
Gene editing technologies, such as CRISPR-Cas9, are also crucial in shaping the future of iPSC differentiation. These tools enable precise manipulation of iPSCs’ genetic makeup, guiding them toward specific lineages and allowing researchers to optimise differentiation protocols, minimising the occurrence of off-target cell types.
Small molecules and signalling pathway modulators are increasingly critical in directing cell fate during differentiation. Researchers are using these chemical tools to exert precise control over cellular processes, enabling the greater accuracy of generating homogeneous populations of desired cell types.
Machine learning algorithms and computational biology are helping to analyse extensive datasets generated from techniques like single-cell RNA sequencing. This data-driven approach helps uncover novel insights into differentiation processes, assisting researchers in refining protocols and identifying critical regulators of cell fate.
Combined with advancements in automation and scale-up techniques, they are pivotal for translating iPSC differentiation protocols into clinical applications. Scalable bioreactors and automated systems enable the production of large quantities of differentiated cells, a crucial aspect for therapies and drug screening on a larger scale.
The differentiation journey in induced pluripotent stem cells (iPSCs) is central to realising their immense therapeutic potential.
With ongoing research and technological advancements, iPSC differentiation is set to achieve more efficient, precise, and scalable differentiation protocols. These developments are poised to revolutionise how we approach various medical conditions and create unprecedented opportunities for personalised medicine.
At NecstGen, we are actively working in the field of iPSC research. To learn how we can help with your development or manufacturing of stem cell and gene therapies, reach out to discuss your challenges.
In these figures, we gathered and visualised overviews of approved ATMPs over the past years for you.
From idea to treatment, you’ll face changing requirement and development challenges. View the figure to see how knowledge of the process inversely relates to freedom to make changes to your process.
Our experts are only a message away to help you understand the impact of any of these aspects and make informed decisions on outsourcing.
We’d be happy to discuss and help you bring cell therapies to patients.

Induced pluripotent stem cells hold immense promise in revolutionising medicine through patient-specific therapies. However, their clinical development presents intricate challenges, including safety validation, differentiation complexities, and ethical considerations to consider.
Induced pluripotent stem cells (iPSCs) represent a significant breakthrough in regenerative medicine, heralding new possibilities for treating diseases once thought incurable.
These versatile cells can potentially treat various health conditions and provide insights into disease mechanisms. The unique characteristic of induced pluripotent stem cells (iPSCs) is that they can be derived from a patient’s cells, enabling researchers to develop disease models. This advances more precise drug testing and the formulation of personalised treatment strategies.
iPSCs are also revolutionising personalised medicine, enabling tailored regenerative therapies and advancing research and development. They facilitate the creation of patient-specific cells for repairing damaged tissues, studying disease, and developing immunotherapies, thus heralding a new era of targeted and effective medical interventions.
While iPSC-based therapies may offer unprecedented opportunities for some of the applications listed above, there are plenty of technical challenges to consider.
Reprogramming somatic cells into iPSCs can introduce unwanted mutations. These genetic aberrations can compromise the functionality and safety of iPSC-derived tissues.
For researchers, the challenge is finding a way of maintaining genetic fidelity throughout the iPSC generation process, while still navigating the need for rigorous quality control measures to minimise the risk of introducing detrimental mutations.
A unique property of iPSCs is their ability to proliferate indefinitely (self-renewal), yet this self-renewal capacity can become a double-edged sword when iPSCs are used for transplantation.
The risk of teratoma formation is concerned with using cells derived from induced pluripotent stem cells (iPSCs), not with the iPSCs themselves. When iPSCs are differentiated into specific cell types before implantation, the challenge lies in ensuring these cells do not proliferate uncontrollably. Balancing cell expansion to prevent unwanted growth is critical to developing safe iPSC-based therapies.
Successfully delivering iPSC-derived cells to target tissues and ensuring their integration within the host environment present substantial hurdles.
Precise delivery and engraftment techniques are critical to maximise the therapeutic benefits of iPSC-based therapies. The challenge lies in achieving the correct location, timing, and interaction with the host tissue.
To compound this further, even when iPSCs are derived from a patient’s cells (autologous iPSCs), immunological responses can still occur when iPSC-derived tissues are transplanted, potentially leading to rejection.
Strategies to enhance graft survival, such as immune modulation and engineering techniques, are being developed to address this nuanced challenge.
Efficiently coaxing iPSCs into desired cell lineages and ensuring their subsequent maturation and functionality is complex. Differentiation protocols must be finely tuned to yield high-quality, functional cells.
Researchers face hurdles in optimising protocols, to prevent suboptimal outcomes that limit the therapeutic potential of iPSC-derived cells.
While induced pluripotent stem cells (iPSCs) possess remarkable and offer prospects for personalised treatments and tissue regeneration, several complexities surround their use. These include issues related to the lack of maturity of iPSC-derived cells, which do not consistently achieve full functionality equivalent to their adult cell counterparts. Additionally, the challenges extend to ensuring the safety, ethical considerations, and control of cell differentiation. As the scientific community progresses in addressing these challenges, iPSC-based therapies may become a cornerstone of patient-specific medical treatments.
In addition to the technical and scientific challenges of iPSCs, there is also a strong need for regulatory and ethical considerations. Stringent regulations are required for approval, as are the ethical considerations that include informed consent and protecting patient well-being.
Rigorous safety assessments through each stage of clinical trials are imperative to address concerns like tumorigenicity, and immunogenicity can only be achieved through clear experimental endpoints with robust release criteria.
Complex ethical debates emerge with the use of iPSCs. Potential modifications using iPSC-derived germ cells raise ethical questions about altering the human genome in ways that could impact future generations. These concerns highlight the need for careful consideration of the long-term effects and the ethical implications of such genomic interventions. The unpredictability of unforeseen long-term consequences associated with iPSC therapies adds further ethical dimensions.
Ethicists, researchers, and policymakers must engage in thoughtful discourse to navigate the promise of iPSCs in medicine with the responsibility to safeguard against unforeseen consequences and maintain ethical integrity.
Contrasting iPSCs with other stem cell modalities reveals a compelling comparative perspective, highlighting the distinct developmental complexities inherent in each approach.
iPSC therapies – while patient-specific and ethically sound – present challenges related to differentiation and tumorigenicity. In contrast, embryonic stem cells (ESCs) offer robust differentiation potential but come with ethical concerns regarding embryo use.
Adult stem cells (ASCs) are less versatile in differentiation but generally raise fewer ethical issues.
To advance the potential of iPSCs, new technologies and techniques must continue to evolve with the latest research.
Ongoing research is driving the evolution of reprogramming methods towards safer and more efficient approaches in regenerative medicine.
This next generation of reprogramming techniques focuses on enhancing safety by reducing the risk of genetic mutations and tumorigenicity associated with iPSCs. Simultaneously, researchers strive for greater efficiency, streamlining the reprogramming process to produce iPSCs more rapidly and precisely.
These advancements promise to accelerate the development of personalised therapies, minimise potential risks, and broaden the scope of iPSC-based treatments. As technology continues to advance, the future of reprogramming holds the potential to revolutionise regenerative medicine.
Integrating iPSCs with therapies like CRISPR-based gene correction opens a realm of unprecedented possibilities in medicine. These synergies leverage the regenerative potential of iPSCs with the precision of CRISPR to address genetic diseases at their roots.
iPSCs can be engineered using CRISPR to correct or replace defective genes, offering patient-specific, customised treatments. This approach holds immense promise for previously incurable genetic disorders.
Furthermore, iPSCs can serve as a renewable source for generating cells for transplantation, enhancing the safety and efficacy of cell-based therapies. The convergence of iPSCs and CRISPR represents a groundbreaking frontier, propelling medicine towards more precise, effective, and personalised therapeutic interventions.
The promise of iPSC therapies is set to revolutionise scientific and medical applications. iPSCs offer hope for countless individuals suffering from diseases once deemed untreatable, signalling a future where personalised medicine could become the standard, not the exception.
Yet, this promise comes with its share of intricacies. The path to realising the full potential of iPSC therapies is a tapestry woven with scientific, ethical, and regulatory aspects, each adding its complexity to the challenge.
At NecstGen, we are dedicated to accelerating safe and effective cell and gene therapy applications. To learn how we can help with your development or manufacturing of stem cell and gene therapies, contact us to discuss your challenges.
In these figures, we gathered and visualised overviews of approved ATMPs over the past years for you.
From idea to treatment, you’ll face changing requirement and development challenges. View the figure to see how knowledge of the process inversely relates to freedom to make changes to your process.
Our experts are only a message away to help you understand the impact of any of these aspects and make informed decisions on outsourcing.
We’d be happy to discuss and help you bring cell therapies to patients.
Organoids have surged to the forefront of biomedical research, revolutionising the field with iPSC technology. These 3D cellular models hold transformative potential for medical breakthroughs and research, propelling our understanding and treatment of complex diseases to unprecedented heights.
Organoids are three-dimensional cell cultures that closely replicate the complex structure and functionality of real organs, bridging traditional two-dimensional cell cultures and living organisms. These miniature, simplified versions of organs are cultivated from stem cells—either pluripotent or organ-specific progenitor cells—that have the extraordinary ability to differentiate into multiple cell types.
The true innovation of organoids lies in their three-dimensional structure, which is essential for cells to interact in a manner that closely resembles their natural environment in the body. This spatial configuration allows the cells to organise themselves into complex, organ-like structures that exhibit multiple functions as human organs, such as contracting like heart tissue or forming neural networks like the brain.
Organoids can be generated to model several organs, including the brain, intestine, liver, kidney, and even the retina. This technology provides a versatile platform for scientists to study a vast array of biological processes and diseases in a controlled setting. This technology is up-and-coming for personalised medicine; organoids derived from a patient’s cells can be used to test how they might respond to different treatments, providing a tailored approach to therapy.
Organoids stand at the confluence of current research and future medical breakthroughs, embodying the promise of what science can achieve when it replicates and harnesses the intrinsic capabilities of human cells.
Deriving organoids from iPSCs is a process derived from the ability of iPS cells to differentiate into any cell type.
iPSCs are coaxed into becoming organoids through a series of carefully orchestrated steps. These begin with the reprogramming of adult cells into iPSCs, followed by exposure to specific signaling cues that guide their development into organ-specific cells.
Researchers use precise combinations of growth factors and 3D culture techniques to encourage iPSCs to form structures that resemble mini-organs, complete with multiple cell types and complex organ-like functionality.
The growth factors and cell culture media used in this process are pivotal in ensuring that iPSCs differentiate into specific types of organoid structures and are used to mimic the cellular signals present during organ development in an organism.
In addition to growth factors and media, scaffolds and matrices provide a 3D framework that offers a substrate for the cells to support the iPSC-derived cells as they grow and organise.
iPSCs have revolutionised the field of regenerative medicine, offering unprecedented opportunities for personalised medicine, disease modelling, drug discovery, and the potential for organ transplantation. Here, we delve into the multifaceted advantages of using iPSC-derived organoids in medical science.
iPSC organoids, which carry the genetic makeup—and potentially the same disease markers as the donor—allow for highly individualised treatment strategies. Physicians can use these organoids to test various drug responses, tailoring treatments specific to the individual’s cellular profile. Such a customised approach could significantly enhance treatment efficacy and minimise adverse effects, opening a new era of patient-centric therapy.
Researchers can replicate disease processes in a controlled laboratory environment by coaxing iPSCs to form organoids that mimic the complexity of human organs. This allows for a deeper understanding of disease pathogenesis at a cellular and molecular level and makes it possible to study with greater precision, potentially revealing novel therapeutic targets.
Organoids provide a more accurate human tissue model for testing the efficacy and safety of new drug compounds, reducing the reliance on animal testing, which often fails to translate to human biology. Furthermore, organoids can help identify toxic side effects early in the drug development process, reducing the costs associated with late-stage drug failures and, more importantly, improving the safety profile of new medications.
Since organoids are derived from a patient’s cells, they could theoretically be used to grow transplantable tissues that are fully compatible with the recipient, virtually eliminating the risk of rejection. While this application is still largely in the research phase, it promises a future where organ shortages are no longer a concern and transplant patients can receive bespoke organs with significantly reduced complications.
Despite their vast potential, some inherent challenges and limitations must be navigated to harness their total scientific and therapeutic value.
iPSC organoids are a monumental step towards replicating human organ structure and function in vitro. However, these miniaturised organ models do not fully recapitulate their full-sized counterparts’ complex architecture and functionality.
Organoids often lack the complete array of cell types found in actual organs, and they typically do not replicate the intricate organ-specific microenvironments, vasculature, and innervation. This incomplete mimicry limits their use as accurate physiological replicas for studying complex organ behaviours or organ replacement therapies.
Another significant hurdle is the high degree of variability observed in iPSC organoid cultures. Factors such as differences in iPSC lines, culture conditions, and organoid generation protocols can lead to inconsistencies in size, shape, and cellular composition.
This variability poses a challenge for standardisation, which is essential for research reproducibility and the potential clinical application of organoids. Developing standardised protocols and benchmarks for organoid generation is crucial to ensure the reliability and comparability of results across studies.
iPSC organoid research also raises ethical concerns, particularly regarding brain organoids. As brain models become more complex and better able to recapitulate aspects of the central nervous system, questions arise about the potential for consciousness or pain perception.
This concern is especially pertinent when organoids exhibit neural activity patterns akin to those of preterm human brains. The ethical implications of creating living models of human organs, the management of patient-derived tissues, and the potential for organoid use in transplantation also raise important questions about consent, the definition of life, and the moral status of these entities.
iPSC organoids herald a new era in medical science, blending the promise of personalised medicine with the rigours of innovative research. These complex 3D cultures mirror the human body more accurately than ever before, offering a dynamic tool for disease modelling, drug discovery, and the prospect of customised organ transplantation.
Yet, the path to successfully implementing organoids is met with many challenges.
For companies looking to navigate the complexities of iPSC organoids, NecstGen can help develop or manufacture stem cell and gene therapies. Reach out to our team, and we will be happy to discuss your challenges.
In these figures, we gathered and visualised overviews of approved ATMPs over the past years for you.
From idea to treatment, you’ll face changing requirement and development challenges. View the figure to see how knowledge of the process inversely relates to freedom to make changes to your process.
Our experts are only a message away to help you understand the impact of any of these aspects and make informed decisions on outsourcing.
We’d be happy to discuss and help you bring cell therapies to patients.
Stem cell research is not without its ethical controversies, primarily around embryonic stem cell use, which involves complex moral and philosophical debates. The advent of iPSCs presents a turning point, promising a less contentious path forward in regenerative medicine.
Whilst prized for their ability to differentiate into any cell type and offering vast potential for treating numerous diseases, embryonic stem cells (ESCs) are mired in ethical controversy, primarily due to the destruction of embryos involved in their procurement.
These concerns stem from the methods of obtaining these cells, which involve the destruction of human embryos, raising questions about the commencement of life and the moral status of an embryo. The debate balances the promise of medical breakthroughs against the inviolability of early human life, fueling an ongoing discourse on the moral bounds of scientific inquiry.
Similar to the isolation and cell culture of embryonic stem cells (ESCs), induced pluripotent stem cells (iPSCs) represent a groundbreaking advancement in regenerative medicine. iPSCs provide a renewable source of human stem cells that can be engineered and differentiated in a laboratory setting. However, it’s important to note that while iPSCs themselves are renewable, the cells differentiated from iPSCs do not typically retain this renewable property.
iPSCs are crafted from adult somatic cells, like skin or blood cells, through a reprogramming process that reverses their state to resemble that of embryonic cells. This process negates the need to use or destroy embryos, thus avoiding the associated ethical concerns of ESC research.
Because iPSCs can be generated from a patient’s own cells, this offers greater options in respect to personalized therapy options and immunological issues.
By reprogramming adult somatic cells to a pluripotent state, iPSCs obviate the need for human embryos – a process that historically necessitated their destruction, sparking significant ethical debate.
This innovation allows scientists to explore the vast potential of stem cells – such as tissue regeneration and disease modeling – without the moral implications tied to embryonic stem cell use. iPSCs thus represent a pivotal shift towards ethically responsible research, ensuring that scientific progress in regenerative medicine advances in harmony with ethical considerations.
iPSCs enable the creation of patient-specific cells that dramatically lower the risk of transplant rejection. This personalized approach not only tailors treatment to the individual’s genetic makeup but also sidesteps ethical issues associated with donor transplants.
Induced pluripotent stem cells (iPSCs) are derived from a patient’s own cells. This approach not only minimizes immunological complications by enhancing the compatibility of transplanted tissues, but it also aligns with ethical standards by avoiding the use of donor cells and tissues. However, the characterization of iPSC therapies as “highly effective” should be clarified; while they hold potential due to their personalized nature, the effectiveness of such therapies can vary and is still under extensive research to confirm their efficacy across various applications.
The process of creating induced pluripotent stem cells (iPSCs) involves reprogramming adult cells to a pluripotent state, thus circumventing the use of fertilized eggs or embryonic cloning. This method is ethically favored as it avoids the creation of new life forms purely for research purposes.
While iPSCs stand as a promising and ethically sound route for scientific advancement, allowing for significant disease modeling and therapeutic development, it is essential to address recent concerns. Some research attempting to mimic early embryonic development stages with iPSCs necessitates a cautious approach in the discourse, ensuring that such studies do not inadvertently cross ethical boundaries associated with reproductive cloning.
iPSC technology enables the development of human cell-based models that closely mimic disease conditions, which could lead to more accurate and ethically responsible science.
This transition offers the twin advantages of potentially boosting the effectiveness of research and addressing animal welfare issues by reducing the dependency on animal testing. Employing human iPSCs for disease modeling allows for a more accurate exploration of human diseases due to species-specific differences; treatments effective in animals, like rodents, may not have the same outcomes in humans. This method signifies a step towards more ethical and representative scientific practices.
iPSC technology has heralded a new era in stem cell research, overcoming some key ethical hurdles by eliminating the need for embryos and enabling patient-specific treatments, thus making regenerative medicine more ethically accessible and personally tailored.
However, challenges persist, including technical complexities and the need for further research to perfect this promising technology.
For companies looking to navigate the complexities surrounding the ethics of iPSCS, at NecstGen we can help with your development and/or clinical testing of stem cell and gene therapies. Reach out to our team and we will be happy to discuss your challenges.
